Utilization of Integrated Child Development Services in India: Programmatic Insights from National Family Health Survey, 2016

 ,
, 
Abstract
:1. Introduction
2. Data and Methods
2.1. Survey Data and Study Population
2.2. Outcomes
2.3. Primary Predictors
2.4. Statistical Analysis
2.4.1. Descriptive Analysis
2.4.2. Econometric Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- NITI Aayog. A Quick Evaluation Study of Anganwadis under ICDS; PEO Report No. 227; Government of India: New Delhi, India, 2015. Available online: https://niti.gov.in/writereaddata/files/document_publication/report-awc.pdf (accessed on 2 May 2020).
- Tandon, B.; Sahai, A.; Vardhan, A. Impact of Integrated Child Development Services on Infant Mortality Rate in India. Lancet 1984, 324, 157. [Google Scholar] [CrossRef]
- Das Gupta, M.; Gragnolati, M.; Ivaschenko, O.; Lokshin, M. Improving Child Nutrition Outcomes in India: Can The Integrated Child Development Services Be More Effective? World Bank: Washington, DC, USA, 2005. [Google Scholar]
- Kapil, U. Integrated Child Development Services (ICDS) scheme: A program for holistic development of children in India. Indian J. Pediatr. 2002, 69, 597–601. [Google Scholar] [CrossRef] [PubMed]
- Kapil, U.; Pradhan, R. Integrated Child Development Services scheme (ICDS) and its impact on nutritional status of children in India and recent initiatives. Indian J. Public Health 1999, 43, 21–25. [Google Scholar] [PubMed]
- International Institute for Population Sciences (IIPS) and ICF; National Family Health Survey (NFHS-4), 2015-16; IIPS: Mumbai, India, 2017.
- NITI Aayog. Nourishing India: The National Nutrition Strategy; Government of India: New Delhi, India, 2017.
- Mamgain, R.P.; Diwakar, G.D. Elimination of Identity-based Discrimination in Food and Nutrition Programmes in India. IDS Bull. 2012, 43, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Thorat, S.; Sadana, N. Discrimination and children’s nutritional status in India. IDS Bull. 2009, 40, 25–29. [Google Scholar] [CrossRef] [Green Version]
- Lokshin, M.; Das Gupta, M.; Gragnolati, M.; Ivaschenko, O. Improving Child Nutrition? The Integrated Child Development Services in India. Dev. Chang. 2005, 36, 613–640. [Google Scholar] [CrossRef]
- Thakur, J.S.; Prinja, S.; Bhatia, S.S. Persisting malnutrition in Chandigarh: Decadal underweight trends and impact of ICDS program. Indian Pediatr. 2011, 48, 315–318. [Google Scholar] [CrossRef]
- Kandpal, E. Beyond Average Treatment Effects: Distribution of Child Nutrition Outcomes and Program Placement in India’s ICDS. World Dev. 2011, 39, 1410–1421. [Google Scholar] [CrossRef]
- Bashir, A.; Bashir, U.; Ganie, Z. Ahmad. Evaluation Study of Integrated Child Development Scheme (ICDS) In District Bandipora of Jammu and Kashmir. Int. Res. J. Soc. Sci. 2016, 3, 34–36. [Google Scholar]
- Jain, M. India’s Struggle Against Malnutrition—Is the ICDS Program the Answer? World Dev. 2015, 67, 72–89. [Google Scholar] [CrossRef]
- Chudasama, R.; Patel, U.; Rangoonwala, M.; Sheth, A.; Vala, M.; Verma, P.; Viramgami, A. Evaluation of Anganwadi centres performance under Integrated Child Development Services (ICDS) program in Gujarat State, India during year 2012-13. J. Mahatma Gandhi Inst. Med. Sci. 2015, 20, 60. [Google Scholar] [CrossRef]
- Dixit, P.; Gupta, A.; Dwivedi, L.K.; Coomar, D. Impact Evaluation of Integrated Child Development Services in Rural India: Propensity Score Matching Analysis. SAGE Open 2018, 8. [Google Scholar] [CrossRef] [Green Version]
- Bose, K.; Biswas, S.; Bisai, S.; Ganguli, S.; Khatun, A.; Mukhopadhyay, A.; Bhadra, M. Stunting, underweight and wasting among Integrated Child Development Services (ICDS) scheme children aged 3–5 years of Chapra, Nadia District, West Bengal, India. Matern. Child Nutr. 2007, 3, 216–221. [Google Scholar] [CrossRef] [PubMed]
- Nayak, N.; Saxena, N.C. Implementation of ICDS in Bihar and Jharkhand. Econ. Political Wkly. 2006, 26, 3680–3684. [Google Scholar]
- Majumdar, M.; Subramanian, S. Capability failure and group disparities: Some evidence from India for the 1980s. J.Dev. Stud. 2001, 37, 104–140. [Google Scholar] [CrossRef]
- A Bhutta, Z.; Black, R.E. Global Maternal, Newborn, and Child Health—So Near and Yet So Far. New Engl. J. Med. 2013, 369, 2226–2235. [Google Scholar] [CrossRef] [Green Version]
- Kerber, K.; E De Graft-Johnson, J.; A Bhutta, Z.; Okong, P.; Starrs, A.; Lawn, J.E. Continuum of care for maternal, newborn, and child health: From slogan to service delivery. Lancet 2007, 370, 1358–1369. [Google Scholar] [CrossRef]
- UNICEF, WHO. Countdown to 2015: Maternal, newborn and child survival. Building a Future for Women and Children: The 2012 Report. Available online: https://reliefweb.int/report/world/countdown-2015-maternal-newborn-child-survival-building-future-women-and-children-2012 (accessed on 2 May 2020).
- Merlo, J.; Wagner, P.; Ghith, N.; Leckie, G. An Original Stepwise Multilevel Logistic Regression Analysis of Discriminatory Accuracy: The Case of Neighbourhoods and Health. PLoS ONE 2016, 11, e0153778. [Google Scholar] [CrossRef] [Green Version]
- StataCorp, L.P. Stata data analysis and statistical Software. Spec. Ed. Release 2007, 10, 733. [Google Scholar]
- Gragnolati, M.; Bredenkamp, C.; Gupta, M.D.; Lee, Y.-K.; Shekar, M. ICDS and persistent undernutrition: Strategies to enhance the impact. Econ. Political Wkly. 2006, 41, 1193–1201. [Google Scholar]
- Deolalikar, A.B. Attaining the Millennium Development Goals in India: Reducing Infant Mortality, Child Malnutrition, Gender Disparities and Hunger-Poverty and Increasing School Enrollment and Completion; Oxford University Press: New Delhi, India, 2005. [Google Scholar]
- Chakrabarti, S.; Raghunathan, K.; Alderman, H.; Menon, P.; Nguyen, P. India’s Integrated Child Development Services programme; equity and extent of coverage in 2006 and 2016. Bull. World Health Organ. 2019, 97, 270–282. [Google Scholar] [CrossRef] [PubMed]
- Balarajan, Y.; Reich, M.R. Political economy of child nutrition policy: A qualitative study of India’s Integrated Child Development Services (ICDS) scheme. Food Policy 2016, 62, 88–98. [Google Scholar] [CrossRef]
- Bhasin, S.K.; Bhatia, V.; Kumar, P.; Aggarwal, O.P. Long term nutritional effects of ICDS. Indian J. Pediatr. 2001, 68, 211–216. [Google Scholar] [CrossRef] [PubMed]
- Allen, L.H.; Gillespie, S.R. What Works? A Review of the Efficacy and Effectiveness of Nutrition Interventions; Asian Development Bank: Manila, Philippines, 2001. [Google Scholar]
- National Council of Applied Economic Research (NCAER). Concurrent Evaluation of the ICDS Program (Vols I and II); NCAER: New Delhi, India, 2001. [Google Scholar]
- Greiner, T.; David, F.P. Nutrition Assessment—India. In Proceedings of the World Bank–UNICEF Joint Nutrition Assessment Workshop, Washington, DC, USA, 11–12 October 2000. [Google Scholar]
- Bhagat, V.M.; Choudhari, S.G.; Baviskar, S.R.; Mudey, A.B. Availability and Utilization of Anganwadi services in an adopted urban area of Wardha. Online J. Health Allied Scs 2015, 14, 4. [Google Scholar]
- Saxena, N.C.; Srivastava, N. ICDS in India: Policy, Design and Delivery Issues. IDS Bull. 2009, 40, 45–52. [Google Scholar] [CrossRef] [Green Version]
- Chaturvedi, A.K. A Study on Training Needs of Anganwadi Worker in Integrated Child Development Services (ICDS) in Sihora Block of Jabalpur District (MP). Ph.D. Thesis, JNKVV, JABALPUR, Madhya Pradesh, India, 2008. [Google Scholar]
- Baker-Henningham, H.; López Bóo, F. Early Childhood Stimulation Interventions in Developing Countries: A Comprehensive Literature Review; Inter-American Development Bank: Washington, DC, USA, 2010. [Google Scholar]
- Rao, N. Preschool Quality and the Development of Children from Economically Disadvantaged Families in India. Early Educ. Dev. 2010, 21, 167–185. [Google Scholar] [CrossRef] [Green Version]
- Thukral, M. Chandrashekhar. Role of anganwadi centers in improving the status of full immunization in Madhya Pradesh. Indian J. Prev. Soc. Med. 2008, 39, 2. [Google Scholar]
- Ahmad, E.; Khan, Z.; Khalique, N.; Amir, A.; Khalil, S. A study of utilization of Integrated Child Development Services in 1-5 years old children registered with rural health training center, Jawan, Aligarh, UP. Indian J. Prev. Soc. Med. 2005, 36, 138–142. [Google Scholar]
- Davey, A.; Davey, S.; Datta, U. Perception regarding quality of services in urban ICDS blocks in Delhi. Indian J. Public Health 2008, 52, 156–158. [Google Scholar]
- Agnihotri, S.P.; Pandey, D.N.; Nandan, D. The impact of rural health services in Agra sub division. Indian J. Public Health 1984, 28, 9–15. [Google Scholar]
- Jain, M.; Nandan, D.; Misra, S.K. Qualitative Assessment of Health Seeking Behaviour and Perceptions Regarding Quality of Health Care Services among Rural Community of District Agra. Indian J. Community Med. 2006, 31, 140–144. [Google Scholar]
- Yadav, A.K.; Jena, P.K. Maternal health outcomes of socially marginalized groups in India. Int. J. Health Care Qual. Assur. 2020, 33, 172–188. [Google Scholar] [CrossRef] [PubMed]
- Gurtoo, A. Addressing utilization of the ICDS programme in Tamil Nadu, India: How class and caste matters. Int. J. Sociol. Soc. Policy 2014, 34, 166–180. [Google Scholar] [CrossRef]
- Ghosh, S.; Das, B.K. Exploring demographic and socio-economic factors influencing utilization of integrated child development services. Asia-Pacific Popul. J. 2013, 26, 11–38. [Google Scholar] [CrossRef]
- Cleland, J.G.; Van Ginneken, J.K. Maternal education and child survival in developing countries: The search for pathways of influence. Soc. Sci. Med. 1988, 27, 1357–1368. [Google Scholar] [CrossRef]
- Wang, W.; Hong, R. Levels and determinants of continuum of care for maternal and newborn health in Cambodia-evidence from a population-based survey. BMC Pregnancy Childbirth 2015, 15, 62. [Google Scholar] [CrossRef] [Green Version]
- Ghuman, S.J. Women’s autonomy and child survival: A comparison of Muslims and non-Muslims in four Asian countries. Demography 2003, 40, 419–436. [Google Scholar] [CrossRef]
- Rai, R.K.; Kumar, C.; Singh, P.K. District level coverage gap in maternal, new born and child health care services in India. J. Epidemiol. Glob. Health 2012, 2, 221–224. [Google Scholar] [CrossRef] [Green Version]
- Rai, R.K. Tracking women and children in a Continuum of Reproductive, Maternal, Newborn, and Child Healthcare (RMNCH) in India. J. Epidemiol. Glob. Health 2014, 4, 239–243. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Service Utilization | Rural | Urban | India | |||
|---|---|---|---|---|---|---|
| Utilization (%) | 95% CI | Utilization (%) | 95% CI | Utilization (%) | 95% CI | |
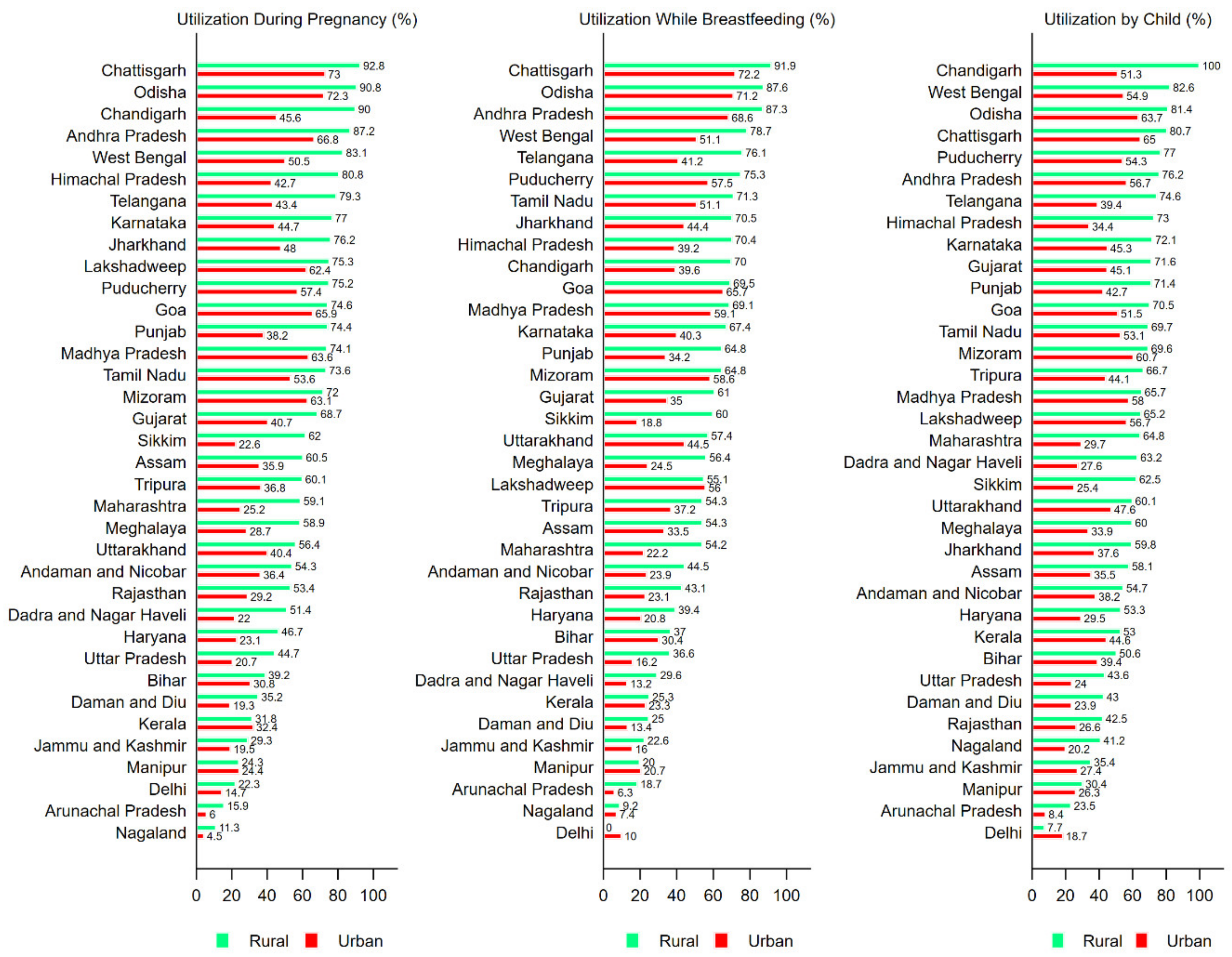
| Mothers During Pregnancy | ||||||
| Any Service | 60.5 | [60.3; 60.7] | 38.8 | [38.4; 39.1] | 54.3 | [54.1; 54.5] |
| Supplementary Food | 57.4 | [57.2; 57.6] | 36.4 | [35.9; 36.7] | 51.4 | [51.3; 51.6] |
| Health Checkup | 47.3 | [47.1; 47.9] | 31.6 | [31.2; 31.9] | 42.8 | [42.6; 43.0] |
| Health and Nutrition Education | 41.9 | [41.7; 42.1] | 29.7 | [29.4; 30.1] | 38.5 | [38.3; 38.6] |
| Mothers While Breastfeeding | ||||||
| Any Service | 55.1 | [54.9; 55.3] | 35.6 | [35.2; 35.9] | 49.6 | [49.4; 49.8] |
| Supplementary Food | 53.1 | [52.8; 53.2] | 33.7 | [33.3; 34.0] | 47.5 | [47.4; 47.7] |
| Health Checkup | 40.5 | [40.4; 40.7] | 28.4 | [28.1; 28.7] | 37.1 | [36.9; 37.2] |
| Health and Nutrition Education | 38.0 | [37.0; 38.2] | 27.6 | [27.2; 27.9] | 35.0 | [34.8; 35.2] |
| By Child < 6 years | ||||||
| Any Service | 59.6 | [59.3; 59.7] | 40.2 | [39.8; 40.1] | 54.1 | [53.8; 54.2] |
| Supplementary Food | 53.1 | [52.9; 53.3] | 35.6 | [35.2; 35.9] | 48.1 | [47.9; 48.3] |
| Health Checkup | 43.2 | [43.0; 43.4] | 30.9 | [30.5; 31.2] | 39.7 | [39.5; 39.9] |
| Immunization | 44.3 | [44.1; 44.5] | 28.6 | [28.2; 28.9] | 39.9 | [39.7; 40.0] |
| Early Child Care | 42.4 | [42.1; 42.7] | 28.2 | [27.7; 28.6] | 38.3 | [38.1; 38.5] |
| Background Characteristics | During Pregnancy | 95% CI | While Breastfeeding | 95% CI | By Child | 95% CI |
|---|---|---|---|---|---|---|
| Rural | ||||||
| Social Group | ||||||
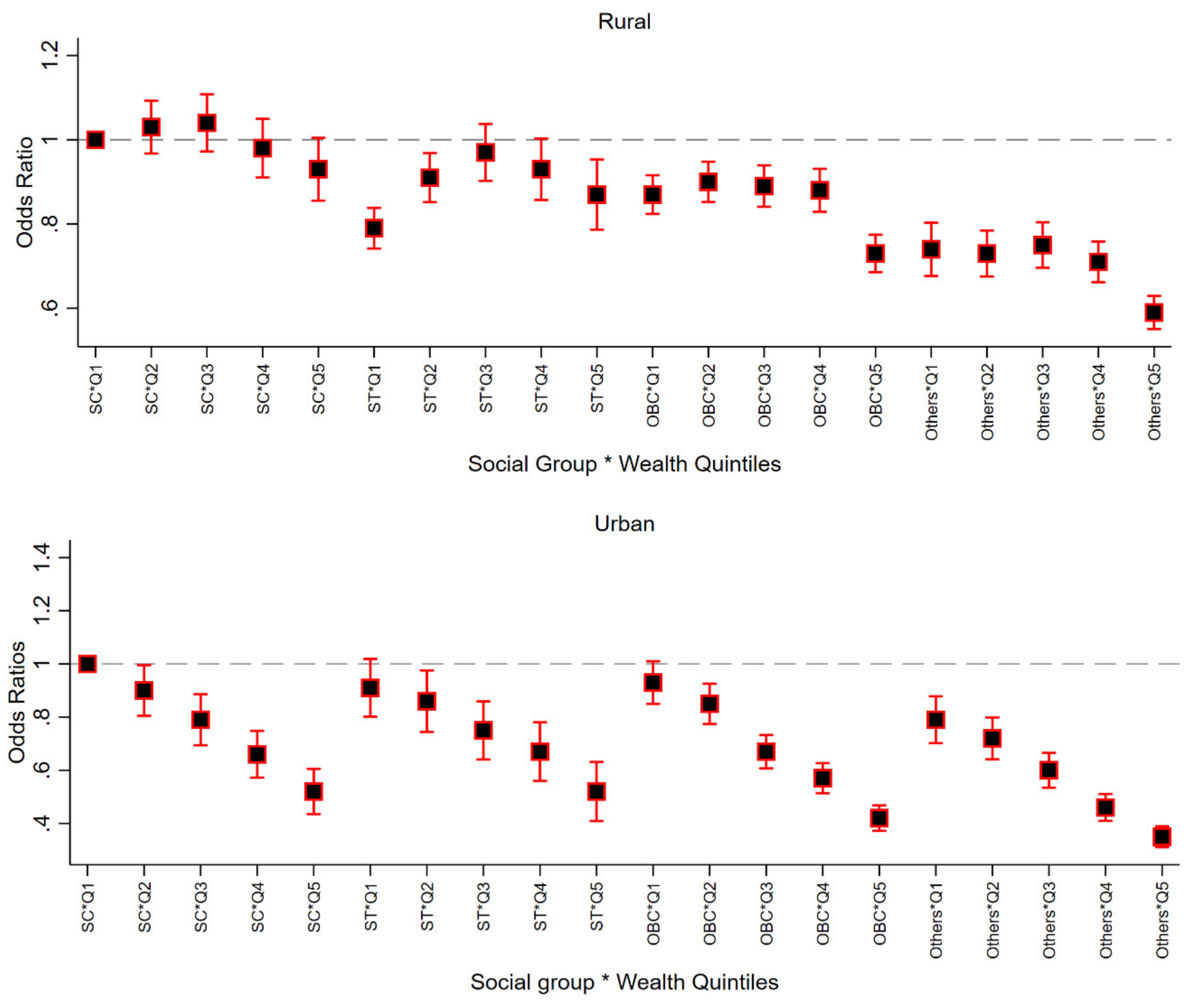
| Schedule Caste | 65.5 | [65.0; 65.9] | 59.7 | [59.2; 60.2] | 63.4 | [62.9; 63.8] |
| Schedule Tribes | 68.9 | [68.6; 69.3] | 64.1 | [63.6; 64.5] | 66.1 | [65.6; 66.4] |
| OBC | 57.7 | [57.4; 58.1] | 52.3 | [51.9; 52.6] | 56.8 | [56.4; 57.1] |
| General | 54.6 | [54.0; 55.1] | 49.4 | [48.8; 49.9] | 56.7 | [56.2; 57.2] |
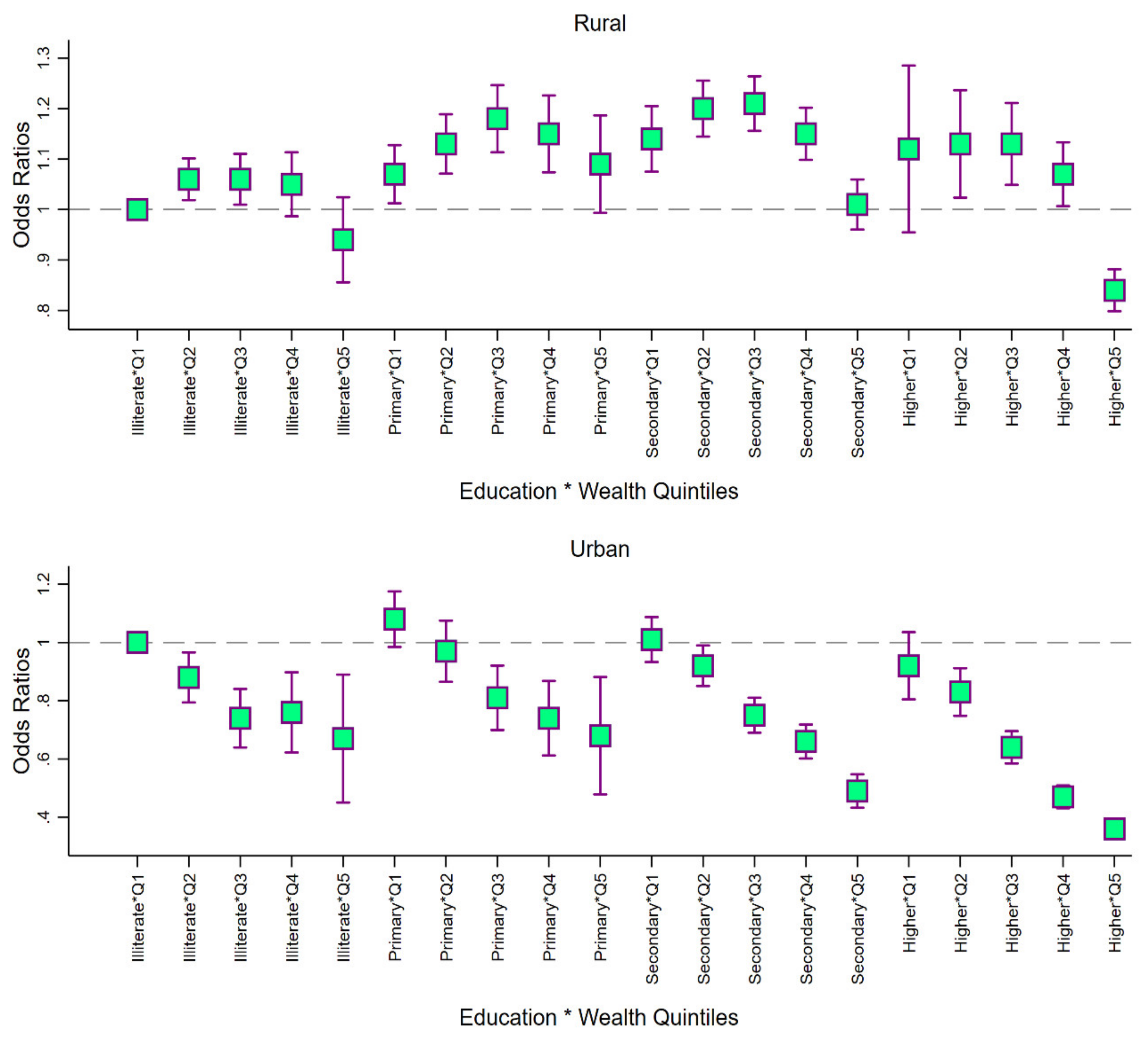
| Wealth Quintile | ||||||
| Lowest | 54.4 | [53.9; 54.8] | 49.8 | [49.3; 50.2] | 54.7 | [54.2; 55.1] |
| Second | 60.8 | [60.3; 61.2] | 55.3 | [54.8; 55.7] | 59.9 | [59.5; 60.4] |
| Third | 65.2 | [64.7; 65.6] | 59.3 | [58.8; 59.7] | 63.0 | [62.5; 63.4] |
| Fourth | 65.7 | [65.2; 66.1] | 60.2 | [59.7; 60.7] | 63.9 | [63.4; 64.3] |
| Highest | 57.8 | [57.3; 58.3] | 52.2 | [51.7; 52.7] | 57.5 | [57.0; 58.0] |
| Religion | ||||||
| Hindu | 62.1 | [61.8; 62.3] | 56.7 | [56.4; 56.9] | 60.7 | [60.4; 60.8] |
| Muslim | 48.9 | [48.4; 49.5] | 44.1 | [46.5; 44.6] | 51.5 | [50.9; 52.0] |
| Others | 67.5 | [66.9; 68.0] | 61.3 | [60.7; 61.9] | 65.1 | [64.5; 65.6] |
| Urban | ||||||
| Social Group | ||||||
| Schedule Caste | 46.2 | [45.3; 47.1] | 42.6 | [41.7; 43.5] | 47.1 | [46.2; 48.0] |
| Schedule Tribes | 50.6 | [49.5; 51.7] | 47.1 | [46.0; 48.1] | 50.9 | [49.8; 51.9] |
| OBC | 41.5 | [40.9; 42.0] | 37.8 | [37.3; 38.4] | 42.4 | [41.8; 42.9] |
| General | 28.9 | [28.2; 25.9] | 26.4 | [25.7; 27.1] | 31.0 | [30.3; 31.7] |
| Wealth Quintile | ||||||
| Lowest | 49.8 | [49.1; 50.5] | 46.3 | [45.6; 47.0] | 50.6 | [49.9; 51.3] |
| Second | 46.6 | [45.7; 47.3] | 42.9 | [42.1; 43.7] | 47.5 | [46.7; 48.3] |
| Third | 38.9 | [38.0; 39.7] | 35.3 | [34.5; 36.1] | 39.9 | [39.0; 40.6] |
| Fourth | 29.7 | [28.9; 30.5] | 27.2 | [26.3; 27.9] | 32.2 | [31.4; 33.0] |
| Highest | 19.8 | [19.1; 20.6] | 17.6 | [16.8; 18.3] | 22.2 | [21.4; 23.0] |
| Religion | ||||||
| Hindu | 40.3 | [39.8; 40.7] | 37.0 | [36.5; 37.4] | 40.8 | [40.3; 41.2] |
| Muslim | 34.4 | [33.7; 35.2] | 31.8 | [31.1; 32.5] | 38.3 | [37.5; 39.1] |
| Others | 38.2 | [37.2; 39.2] | 33.2 | [32.2; 34.3] | 40.4 | [39.2; 41.4] |
| All India | ||||||
| Social Group | ||||||
| Schedule Caste | 60.9 | [60.5; 61.3] | 55.7 | [55.2; 56.1] | 59.5 | [59.1; 59.9] |
| Schedule Tribes | 66.7 | [66.3; 67.0] | 61.9 | [61.6; 62.4] | 64.2 | [63.7; 64.5] |
| OBC | 53.1 | [43.8; 44.6] | 48.2 | [47.8; 48.5] | 52.7 | [52.3; 52.9] |
| General | 44.2 | [43.8; 44.6] | 40.1 | [39.6; 40.5] | 46.3 | [45.9; 43.7] |
| Wealth Quintile | ||||||
| Lowest | 55.5 | [55.1; 55.8] | 50.8 | [50.5; 51.2] | 55.6 | [55.2; 55.9] |
| Second | 62.3 | [61.9; 62.8] | 56.6 | [56.2; 56.9] | 61.1 | [60.7; 61.4] |
| Third | 61.3 | [60.9; 61.7] | 56.4 | [55.9; 56.7] | 59.9 | [59.4; 60.2] |
| Fourth | 52.2 | [51.8; 52.6] | 47.6 | [47.1; 48.0] | 52.3 | [51.8; 52.7] |
| Highest | 34.1 | [33.6; 34.5] | 30.7 | [30.2; 31.1] | 35.8 | [35.3; 36.2] |
| Religion | ||||||
| Hindu | 56.4 | [56.2; 56.6] | 51.5 | [51.3; 51.8] | 55.5 | [55.3; 55.7] |
| Muslim | 43.1 | [42.7; 43.6] | 39.2 | [38.7; 39.6] | 46.2 | [45.7; 46.6] |
| Others | 58.1 | [57.6; 58.7] | 52.3 | [51.8; 52.8] | 57.2 | [56.7; 57.6] |
| Beneficiaries | Rural | Urban | India | |||
|---|---|---|---|---|---|---|
| Percent | N | Percent | N | India | N | |
| At all three points | 42.4 | 95,164 | 26.7 | 18,839 | 37.9 | 111,888 |
| By mother during pregnancy and by child | 6.1 | 13,610 | 3.9 | 2768 | 5.5 | 16,089 |
| By mother during pregnancy and breastfeeding | 8.5 | 19,056 | 5.5 | 3849 | 7.6 | 22,496 |
| By mother during breastfeeding and by child | 2.5 | 5683 | 2.0 | 1386 | 2.4 | 6992 |
| By child only | 1.5 | 3288 | 1.2 | 875 | 1.4 | 4133 |
| By mother only while breastfeeding | 8.6 | 19,396 | 7.7 | 5404 | 8.4 | 24,668 |
| By mother only during pregnancy | 3.6 | 8134 | 2.8 | 1960 | 3.4 | 9979 |
| None | 26.8 | 60,273 | 50.3 | 35,555 | 33.5 | 98,995 |
| Total | 100 | 224,604 | 100 | 70,636 | 100 | 295,240 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rajpal, S.; Joe, W.; Subramanyam, M.A.; Sankar, R.; Sharma, S.; Kumar, A.; Kim, R.; Subramanian, S.V. Utilization of Integrated Child Development Services in India: Programmatic Insights from National Family Health Survey, 2016. Int. J. Environ. Res. Public Health 2020, 17, 3197. https://doi.org/10.3390/ijerph17093197
Rajpal S, Joe W, Subramanyam MA, Sankar R, Sharma S, Kumar A, Kim R, Subramanian SV. Utilization of Integrated Child Development Services in India: Programmatic Insights from National Family Health Survey, 2016. International Journal of Environmental Research and Public Health. 2020; 17(9):3197. https://doi.org/10.3390/ijerph17093197
Chicago/Turabian StyleRajpal, Sunil, William Joe, Malavika A. Subramanyam, Rajan Sankar, Smriti Sharma, Alok Kumar, Rockli Kim, and S. V. Subramanian. 2020. "Utilization of Integrated Child Development Services in India: Programmatic Insights from National Family Health Survey, 2016" International Journal of Environmental Research and Public Health 17, no. 9: 3197. https://doi.org/10.3390/ijerph17093197