
Abstract
Ratio-based prevalence and absolute headcounts are the two most commonly accepted metrics to measure the burden of various socioeconomic phenomenon. However, ratio-based prevalence, calculated as the number of cases with certain conditions relative to the total population, is by far the most widely used to rank burden and consequently for targeting, across different populations, often defined in terms of geographical areas. In this regard, targeting areas exclusively based on prevalence-based metric poses certain fundamental difficulties with some serious policy implications. Drawing the data from the National Family Health Survey 2015–2016, and Census 2011, this paper takes four indicators of child undernutrition in India as an example to examine two contextual questions: first, does the choice of metric matter for targeting areas for reducing child undernutrition in India? and second; which metric should be used to facilitate comparisons and targeting across variable populations? Our findings suggest a moderate correlation between prevalence estimates and absolute headcounts implying that choice of metric does matter when targeting child undernutrition. Huge variations were observed between prevalence-based and absolute count-based ranking of the districts. In fact, in various cases, districts with the highest absolute number of undernourished children were ranked as relatively lower-burden districts based on prevalence. A simple comparison between the two approaches—when applied to targeting undernourished children in India—indicates that prevalence-based prioritization may miss high-burden areas where substantially higher number of undernourished children are concentrated. For developing populous countries like India, which is already grappling with high levels of maternal and child malnutrition and poor health infrastructure along with intrinsic socioeconomic inequalities, it is critical to adopt an appropriate metric for effective targeting and prioritization.
Similar content being viewed by others
1 Introduction
Identification and prioritization of target areas across populations is a fundamental task in policymaking. Ratio-based prevalence (P from hereafter), calculated as the number of cases with certain conditions relative to the total population, is by far the most widely used metric to rank the burden across different populations, often defined in terms of geographical areas (Davis and Hertz 1951; Minhas 1974; Dandekar and Rath 1971; Sen 1976; Arriaga 1970). Based on P, areas with a relatively higher prevalence of poor conditions, related to measures ranging from poverty (Minhas 1974; Dandekar and Rath 1971; Sen 1976), illiteracy (Carr-Hill and Pessoa 2008), unemployment, urbanisation (Arriaga 1970; Davis and Hertz 1951), morbidity, disability, and malnutrition (United Nations Children’s Fund 2012), are more likely to be prioritized for immediate interventions and greater resource allocation. For instance, the ranking of countries based on the Global Hunger Index is primarily derived from P of child undernutrition (i.e. child stunting and wasting) (von Grebmer et al. 2018), and countries like Burundi and Democratic Republic of Congo with high P of child stunting are labelled as priority areas. India is also considered as a priority area given the high prevalence of wasting in South Asia (von Grebmer et al. 2018). Similarly, comparisons of disease burden across geographical regions and population groups are predominantly based on P metric (James et al. 2018).
However, targeting areas exclusively based on P poses two fundamental difficulties. First, P, derived as a ratio relative to the total population, does not consider the absolute size of the total population. To illustrate this problem with a hypothetical example, consider two areas X and Y with total child populations of 100 (N(X)) and 1000 (N(Y)) respectively and an equivalent P of stunting such that P(X) = P(Y) = 20% (Box 1). Based on P, it appears that the stunting burden in X and Y is the same. However, the absolute number (A from hereafter) of affected children in Y (A(Y) = P(Y) * N(Y) = 0.2 * 1000 = 200) is ten times higher than that in X (A(X) = P(X) * N(X) = 0.2 * 100 = 20).
Second, P violates what is known as the ‘constituency principle’ in the literature of population ethics (Broome 1996; Subramanian 2002). Simply, the ‘constituency principle’—in terms of the above example—states that any increase in the number of non-stunted children should have no effect on the extent of stunting measure of a given population. To demonstrate this problem, let us assume that N(X) is increased by 100 non-stunted children (so now N(X) = 100 + 100 = 200) and thus the P(X) is reduced to 20/200 * 100 = 10%. Simply adding non-stunted children in area X automatically reduces the P(X) leading to a false conclusion that stunting has halved even though nothing has been done to treat stunted children in the area. In contrary, A measures do not encounter this problem associated with ‘constituency principle’.
While A has certain advantages as a metric to rank and compare the extent of diverse social, economic, and population health burden, A does not comply with the underlying intuition related to ‘probability principle’ (Subramanian 2002). Intuitively, a metric for measuring the extent of child stunting in an area should also be associated with the likelihood of encountering a stunted child in that area. However, this notion of “likelihood” is completely missed by A. For example, considering information from Box 1, the burden of stunting in area U is higher than T when compared on the basis of A (Since A(U)= 150 > A(T)= 30). However, the probability of encountering a stunted child in area T is much higher (30%) than in area U (15%). Therefore, when considering the ‘probability principle’, it would not be entirely correct to argue that the burden of stunting in area U is higher than in T, even though the likelihood of finding a stunting child is double in area T than in U.
In summary, the commonly used P upholds the “likelihood principle” but falls short in respect to the ‘constituency principle’; on the other hand, A does not violate the ‘constituency principle’ but is not in compliance with ‘likelihood principle’. Therefore, exclusive reliance on either one of these metrics is not viable as each one on its own can reverse the policy implication entailed by the other.
This tension between the use of P and A (or both) has been discussed in a few studies, mostly in the paradigm of poverty measurement and inequality (Arriaga 1970; Subramanian 2002, 2005; Chakravarty et al. 2002; Broome 1996; Krtscha 1994). In his seminal work on gauging urbanization, Arriaga (1970) was the first to note the conflicting properties of the two metrics, thereby stressing the need to account for not only the proportion of urbanised population, but also the absolute size of the urban population in any proper reckoning of the ‘degree of urbanization’. In the literature on measuring poverty and distributional inequalities across various populations, a couple of scrutinized measures were proposed to incorporate both “Constituency and Likelihood Principles”—a case for taking both probability and size into consideration (Subramanian 2002, 2005; Hassoun and Subramanian 2012; Zoli 2003, 2009; Mukherjee 2008; Chakravarty et al. 2002). In a recent paper, Subramanian and Mukherjee (2018) constructed an intuitively plausible intermediate measure of poverty - i.e. Mixed Index (M hereafter)—which is a geometric mean of P and A and is given by M = (PA)1/2 (Subramanian and Mukherjee 2018). A relevant property of index M is that when poverty comparisons are tied in terms of P, the tie can be broken by A; and when they are tied in terms of A, the tie can be broken by P. Besides, in situations when poverty ranking distributions by P can be inverted by A, it is useful to have an adjudicator (M index) between the claim of the two indices.
In the same vein, studies have also argued that the choice of metric has considerable relevance for targeting as well as distribution of resources for poverty reductions (Besley and Kanbur 1991; Kanbur 2001). Despite its non-trivial implications, the relevance of choice between P and A for comparisons and targeting has not received much analytical attention in health and development. In fact, nutrition policies in developing countries like India still rely solely on P for targeting and prioritizing focus areas (NITI 2018). For instance, the Government of India has recently identified 115 ‘Aspirational Districts’ (AD) based on P measures of several socioeconomic indicators classified under 6 broad themes (NITI 2018). It is presumed that reductions in P would lead to improvement in India’s human development rankings. However, improvements in P can make greater impact on human development if these ADs also have high share of population as captured by metric A. Similarly, India’s flagship nutrition programme ‘POSHAN Abhiyaan’ also focuses on P metric for selecting the priority 315 districts under phase-I of its implementation. In this context, two questions immediately arise: first, does the choice of metric matter for targeting policy areas for child undernutrition in India? and second; which metric should be used for facilitating comparisons and targeting across variable populations? If P is employed as the primary basis for any type of ‘indirect targeting’, it will disregard the constituency principle, and if policy targeting is solely based on A, it will ignore the likelihood principle.
This paper takes four indicators of child undernutrition in India as an example to assess the differentials in district ranking (policy priority) by three metrics of P, A, and M to illustrate the importance of the choice of metric in identifying priority areas. At this point, it is worth pointing out that this study is an empirical exercise based on existing metrics (i.e. P, A and M) to compare the districts ranking in India by taking POSHAN Abhiyaan target variables viz. child stunting, underweight, low birth weight (LBW hereafter), and anemia. More specifically, the paper examines the correlation between estimates from the three approaches (P, A, and M) to unravel whether the targeted areas (or districts) are consistent with these metrics.
2 Methods
2.1 Survey Data and Study Population
The study utilizes data from the most recent round of the National Family Health Survey (NFHS), 2015–2016 and Census of India, 2011. The sampling frame for NFHS 2016 was based on Census 2011 providing estimations on all available indicators for 640 districts from all states and Union Territories (UTs) by rural and urban areas separately. Data in NFHS were obtained from a two-stage stratified random sampling frame. The villages (for rural areas) and Census Enumeration Blocks (for urban areas) served as primary stage unit. In the second stage, households were selected for survey from each cluster/village/block on the basis of probability systematic sampling. The final analytic sample after excluding missing and flagged information on child’s age, sex, height and weight was 225,002 children aged 0–59 months for stunting, underweight, LBW and wasting and 208,608 children aged 6–59 months for anemia. In addition, total child population (0–59 months) was taken from Census 2011.
2.2 Child Undernutrition Indicators
This study primarily analyses four nutritional outcomes among children: stunting, underweight, anemia, and LBW. Three anthropometric measures were constructed based on the WHO child growth reference standards (WHO 2006). The NFHS provides standard information on child’s height and weight. The weight was measured by skilled health investigators using digital solar-powered scales along with adjustable short measuring boards. While standing height was taken for children aged 24–59 months, recumbent length was measured in case of younger children below the age of 24 months (IIPS and ICF 2017). The raw height and weight measures were transformed into age- and sex-specific z-scores using WHO child growth standards (WHO 2006). A child’s “height for age” (or “weight for age”) is a measure of their height (or weight), relative to a standard (healthy) population of the same sex and same age (in months). It is expressed as the difference between the height of the observed child and the average height of healthy children i.e. z-scores, scaled by standard deviation (SD) of child’s height of healthy population. Stunting was defined as height-for-age z-scores less than − 2 SD, underweight as weight-for-age z-scores less than − 2 SD, and wasting as weight-for-height z-scores less than − 2 SD. Anemia among children aged 6–59 months was measured as a binary outcome (Yes = 1/No = 0) taking 11.0 gm/dl of haemoglobin level as a threshold (IIPS and ICF 2017). Further, binary variable was constructed for children with LBW (Yes = 1/No = 0) defines as those with written record of birthweight less than 2.5 Kgs.
2.3 Statistical Analysis
2.3.1 Prevalence (P)
We calculated the P (%) of child stunting, underweight, wasting, anaemia and LBW at the national, state, and district levels directly from NFHS 2016 data. The metric P was calculated as the ratio of number of children with nutritional failure (q) to total children (n) at a particular area (j): \(\left( {P_{j} = {\raise0.7ex\hbox{${q_{j} }$} \!\mathord{\left/ {\vphantom {{q_{j} } {n_{j} }}}\right.\kern-0pt} \!\lower0.7ex\hbox{${n_{j} }$}}*100} \right)\).
2.3.2 Absolute Headcount (A)
To put it simply, A = q (i.e. total number of children with nutrition failures). The A at national, state and district level is calculated by multiplying P estimated from NFHS 2016 by the total child population (0–5 years) available from Census 2011. Here, we simply used the product of prevalence ratios (provided by NFHS 2016) and absolute total children (aged 0–5 years) (provided by Census 2011) to arrive at district-level estimates of A.
2.3.3 Mixed Index (M)
We used Mixed index proposed by Subramanian and Mukherjee (2018) to measure child undernutrition (stunting, underweight, wasting, anemia and LBW) which takes both probability and size into consideration (Subramanian and Mukherjee 2018). Taking stunting as an example, let \(d_{i} \in \{ 0,1\}\) be the nutritional status of any child i in some given location. If \(d_{i} = 0\), child i is not stunted; if \(d_{i} = 1\), child i is stunted. If there are q stunted children in a population of n children in this location, then the probability \(p_{i}\) that any child i chosen at random in the location is stunted is given by \(p_{i} = q/n,\) where q/n, of course, is the P. The expected value of stunting in the location under consideration—call it M (Mixed Index)—is simply a probability weighted sum of individual deprivation statuses, that is:
The measure M can thus be usefully interpreted as the expected value of stunting in a locality, which takes account of both likelihood (P) and size considerations (A); as such, it serves as an intuitively plausible intermediate measure of prevalence (Subramaniam and Mukherjee 2018). It is worth mentioning here that for computing M, we used P as the ratio (and not %), and A in millions.
To further identify the priority areas, districts were ranked based on all three metrics (P, A and M) separately (where higher ranks indicate higher burden) and presented via two-way cross tables. The P estimates were computed using sampling weights as provided by NFHS 2016 for descriptive analysis. We further assessed the correlation between metrics at the district and state levels via scatter plots, Pearson correlation coefficient and Spearman rank correlation coefficient. To further understand the disagreement between the metrics, we classified all 640 districts by quintiles based on three metrics separately for all 4 nutritional failures. Finally, we investigated how the priority districts identified under two current Government of India’s (GOI hereafter) schemes (i.e. ADs and POSHAN Abhiyaan) vary from those that were identified on the basis of our P, A, and M estimates. We also compared the cumulative share of undernourished children targeted under ADs and POSHAN Abhiyaan, and by P, A and M.
Lastly, we computed a Moran’s I Index, which is an autocorrelation coefficient that tests how likely geospatial clusters could have appeared by chance. It takes values between − 1 and 1; the closer the index is to − 1 (dispersed) or + 1 (clustered), the stronger the association. We defined a geospatial cluster, or neighbourhood, as a set of contiguous districts that share boundaries with other districts. Specifically, we used a “rook” definition which is a more stringent contiguity definition than a “queen” where neighbours can be defined as districts that touch at a single point. Not all neighbourhoods were of the same size. After defining neighbourhoods, we computed the average prevalence (prevalence lag) and count (count lag) of each neighbourhood cluster. We performed a Monte Carlo test where prevalence lag and count lag values were randomly assigned to spatial polygons in our dataset, and for each permutation, a Moran’s I value was computed as:
where \(N\) is the number of polygons (districts in this case), \(x_{i}\) is prevalence or count, \(\bar{x}\) is average prevalence or count, \(w_{ij}\) is a matrix of spatial weights, and \(W\) is the sum of all \(w_{ij}\). We then compared our observed Moran’s I to the sampling distribution of bootstrapped Moran’s I where the null hypotheses were that both prevalence lag and count lag are randomly distributed across the polygons. The estimates for child stunting, underweight, anemia and LBW is presented as primary results—given these four are the key policy outcomes under POSHAN Abhiyaan—, whereas estimates for child wasting is presented as supplementary. All the analyses were performed using Stata (version 15.0) (25) and mapping was done “spdep” package in R 4.0 (Bivand and Wong 2018).
3 Results
The mean P of child stunting at the national level was 38.37% and it ranged from 13.12 to 65.20% across 640 districts in India with a SD of 9.94% (Table 1; district estimates provided in Supplementary Tables S1-S5). About 35.73% of total children were estimated to be underweight ranging from a minimum 6.33% to maximum 60.34% with a SD of 11.71% across districts. The overall P of LBW was 22.01% with a SD of 6.01% across all districts ranging from 2.02 to 43.6%. At national level, the P of anemia among children (6–59 months) was 58.41% and at district level the P ranged by 78.78%. Based on A measure, we found on average A(stunting)= 93,394 children, A(underweight)= 84,976 children, A(LBW)= 40,062 and A(anemia)= 143,148 children, with substantial variation across districts. The mean value of M for stunting across 640 districts range from 0.107 to 0.482 with the mean value of 0.160. Similarly, based on M, average value for M(underweight)= 0.148; M(LBW)= 0.213; and M(anemia)= 0.245, with noticeable variations across districts.
The scatter plots between P (in %) and A of children with anthropometric failures, LBW and anemia elicit a moderate correlation (Fig. 1). Across all districts, there was a moderate to low correlation between P and A measures for stunting (r = 0.55; Spearman’s rank r = 0.597), underweight (r = 0.55; Spearman’s rank r = 0.667), anemia (r = 0.455; Spearman’s rank r = 0.535), and LBW (r = 0.473; Spearman’s rank = 0.502). When comparing the maps in Figs. 2 and 3, notable distinction in the distribution pattern of child undernutrition can be observed between P and A across all districts. For instance, Panel A (in Fig. 2) suggest that most of the districts in Gujarat falls in lowest quintile (blue shade) of stunting based on P, whereas, on the basis of A (Panel A in Fig. 5) reveals that same districts fall in the fourth quintile of stunting. These observations were consistent for other indicators (underweight LBW, and anemia) as well.

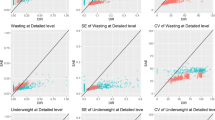
Scatter plot: correlation between prevalence (%) of child anthropometric failures and absolute number of children with failures by districts, India, NFHS 2016. Note: Absolute number of children estimated indirectly using Census 2011; r = Pearson correlation coefficient; r(s) = Spearman Rank correlation coefficient. Estimates are *significant at 0.10 ** at 0.05 level *** at 0.01 level

Prevalence (%) of a stunting, b underweight, c LBW and d anaemia across 640 districts, India, NFHS, 2016 in children (0–59 months)

Absolute number of children (0–59 months) across districts, India, NFHS, 2016 for a stunting, b underweight, c LBW and d anaemia
In the same vein, we also estimated Moran’s Indices to understand the spatial distribution of prevalence and absolute count of children with nutrition failures across districts in India. The estimates elicit a noticeable difference in the spatial distribution (clusters) of failures between two metrics (Table 2). For example, the value of Moran’s I for distribution of prevalence of stunting across districts was 0.45 (p < 0.001), whereas for absolute number of stunted children, it was 0.32 (p < 0.001). This clearly indicates that prevalence numbers are spatially more clustered than absolute numbers. The difference is much higher for underweight where the value of Moran’s coefficient is 0.59 (p < 0.001) for prevalence, and 0.29 (p < 0.001) for absolute count. Similar differences were observed for children with LBW, and anemia (Table 2).
Figure 4 reveals that M index values across districts are significantly correlated with P (%) in case of stunting, and underweight. For example, the Pearson’s correlation coefficient was 0.726 (p < 0.001) and 0.773 (p < 0.001) for stunting and underweight respectively. Similarly, Spearman’s rank correlation coefficient was 0.735 (p < 0.001) for stunting and 0.797 (p < 0.001) for underweight. A moderate correlation was observed between M and P in case of LBW and anemia. The Pearson’s and Spearman’s rank correlation coefficient value for anemia was estimated at 0.674 (p < 0.001) and 0.679 (p < 0.001) respectively. In the same vein, a very high and positive correlation was observed between M index values and A across districts for all the nutritional failures (Fig. 5). The value of Pearson’s correlation coefficient between M and A for child stunting and underweight was 0.954 (p < 0.001) and 0.942 (p < 0.001) respectively. Further, in case of child LBW (r = 0.957; Spearman’s rank r(s) = 0.990) and anemia (r = 0.942; Spearman’s rank r(s) = 0.958) as well, the correlation between M and A was very high.

Scatter plot: correlation between prevalence (%) of child anthropometric failures and Mixed Index by districts, India, NFHS 2016. Note: r = Pearson correlation coefficient; r(s) = Spearman Rank correlation coefficient. Estimates are *significant at 0.10 ** at 0.05 level *** at 0.01 level

Scatter plot: correlation between absolute number of children with nutritional failures (in millions) and Mixed Index by districts, India, NFHS 2016. Note: absolute number of children estimated indirectly using Census 2011; r = Pearson correlation coefficient; r(s) = Spearman Rank correlation coefficient. Estimates are *significant at 0.10 ** at 0.05 level *** at 0.01 level
The quintile distribution of districts further reveals stark difference between the three metrics (P, A, and M) for all four child nutritional failures (Table S6). In case of child stunting, quintile categories based on P and A were different for about 420 districts (65%). In fact, some districts (for example Pune) were in first quintile based on P and in fifth quintile based on A. Similarly, in case of underweight and anemia, about 401 districts and 441 districts were not in same quintile categories based on P and A. When compared between P and M, about 357 districts and 409 districts were classified under different quintile categories for stunting and LBW respectively. However, about 134 districts (for stunting) and 150 districts (for underweight) were not in same quintiles based on A and M.
3.1 Comparing District Ranking by P and A
Striking differences were observed in the rank ordering of districts based on P, A and M of child stunting (Table S1). For instance, Thane (of Maharashtra), with the largest number of stunted children, ranked the lowest (640) in terms of A (429,316 children), whereas it ranked 387 in terms of P (39%). Based on M, Thane (0.409) was ranked 633 for child stunting. Similarly, Dibang Valley (of Arunanchal Pradesh) ranked 314 based on P (35.6%) but had the least number of stunted children (327) across all 640 districts. Further, Ernakulam was ranked first on the basis of lowest prevalence of stunting (13.1%). However, on the basis of A (34,035 children) and M (0.067) it was ranked 195 and 101 respectively. Of the bottom 20 districts ranked based on P (%), only 5 districts (20%) overlapped with those among the bottom 20 based on A. Similar contrast in ranking was observed in case of Sheopur district between P, A and M. Sheopur ranks 617th based on P, however on the basis on the basis of A, it ranked much below at 217 and on the basis of M, it was ranked 363. Also, while the bottom 132 districts by A accounted for about 50% of total stunted children, the total share of the same numbers by P accounted for about 35% of total stunted children.
Further, district ranking by P of underweight varied substantially from district ranking by A and M of underweight children (Table S2). For example, Paschimi Singh Bhumi had the highest P of underweight (66.7%, rank = 640), but ranked 551 by A with estimated 147,342 underweight children and 613 by M with index value of 0.313. With the largest number of underweight children (449,878), Thane ranked 640 in terms of A and M (0.429), whereas it ranked 451 in terms of P (40.9%). Further, while Sheopur ranked 635th on the basis of P with the underweight prevalence of 55.9, it ranked 300th on the basis of metric A with 55,339 underweight children and 395 on the basis of metric M with the index value of 0.175. Of 640 districts, about 20% of them ranked on the basis of P (bottom 133 districts) accounted for less than 31% of total underweight children in India. On the other hand, targeting bottom 133 districts by A covered about 51% of total underweight children in India. A similar pattern was observed for LBW (Table S3). While Mandsaur ranked the lowest with P(LBW) of 43.6%, it ranked 527 in terms of A, and 583 in terms of M. Another district, Thane, ranked the last (640) in terms of A of LBW children (227,690), but stood at the 461st position when ranked by P (20.7%). Further, Vaishali district of Bihar ranks 513 on the basis of A with 60,108 number of LBW children, and 473 on the basis of M (0.271), whereas in terms of P, it ranks 92 with the prevalence of 11.90%. This clearly shows that the rank ordering of districts varies substantially across metrics (i.e. P, A, and M) in case of LBW also.
The largest difference in district ranking between P and A was seen for anemia among children aged 6–59 months (Table S4). With the highest P(anemia) of 84.4%, Banswara ranked 640 in terms of P, but ranked 547 in terms of A with 232,667 anemic children. While A(anemia) was the highest in Thane (606,885), it ranked above 300 districts by P(anemia). Similarly, Purba Champaran ranks 638 by A with 552,825 anemic children, whereas, based on P, it ranks 446 with the anemia prevalence of 65.9%. Importantly, only 5 districts overlapped out of the bottom 50 districts ranked by P and A, indicating that about 90% of identified burden areas are different depending on the choice of metric. This shows that the choice of metric (here between P and A) can potentially inverse the ranking of districts and therefore can affect the allocation of resources among priority areas. These differences in rank ordering across metrics were also evident in case of child wasting as well (Table S5).
3.2 Discordance with Aspirational Districts
The ADs has a focus on six different development domains including nutrition.We computed cumulative share of total undernourished children targeted under the current priority 115 ADs and compared those by estimating the same through alternative metrics (i.e. P, A and M) (Table 3). The current focus on 115 ADs is estimated to cover about 20.4% (10.9 Million) of total stunted children, whereas if the same priority is based on A, the worst 115 districts will cover about 45.8% (24.3 Million) of total stunted children in India. Similarly, if the priority is to be based on index M, the bottom 115 districts will cover an additional 12.8 million stunted children than actual 115 ADs.
Similarly, in the case of underweight, bottom 115 districts by A and M will cover about 45% of total underweight children, which is more than twice the coverage under current 115 ADs (20.5%). Further, the current ADs account for about 17.2% (4.4 Million) of total LBW children in India. However, priority 115 districts based on A and M covers about 45.3% (11.6 Million) and 44.5% (11.4 Million) of total LBW children respectively. This difference between target coverage is even higher in case of child anemia. For instance, the priority 115 districts based on A covers about 20.4 Million more anemic children (a difference of 25.6 percentage points) compared to target coverage under current 115 ADs.
More eloquently, figure S1 via maps depicts the discordance between targeted 115 ADs and worst 115 districts by P given the very few common districts (marked in red colour). Similarly, figure S2 reveals a very few overlapping districts (in red) between targeted ADs and 115 high burden districts by A. More specifically, 39 districts are common between 115 ADs and 115 high burden districts by P of stunting (Table S7). On the other hand, only 21 districts are common when 115 ADs were compared with 115 high burden districts by A for stunting (Table S5). Also, districts common across all three approaches (i.e. ADs, P and A) are scant (marked in black) (Figure S5). However, it may be noted that these common districts deserve top priorities as they reveal high burden of child undernutrition by all metrics. About 16 districts are common (across all three metrics i.e. ADs, P and A in case of stunting, 10 districts in case of underweight, 4 districts in case of LBW, and 3 districts in case of anemia (Table S7). This depicts that discordance among metrics is relatively higher in case of anaemia compared to other outcomes.
3.3 Discordance with Priority Districts (Phase-1) under POSHAN Abhiyaan
We also compared the target coverage based on priority 315 districts (under phase 1) of POSHAN Abhiyaan with the alternative targeting numbers based on bottom 315 districts ranked by A and M (Table 3). The current phase 1 districts target about 67.5% of total stunted children in India; however, this coverage would increase by 14% if ranking had been based on A or M. Similarly, the number of underweight children covered under current 315 districts (32.9 Million) is substantially lesser than what would have been targeted when prioritized by A (40.6 Million). Also, in the case of anemia, the bottom 315 districts based on A account for nearly 81% of total anemic children, whereas the current 315 identified districts cover 62.4%. Finally, for LBW, rank ordering based on A and M will cover about 80.5% (20.6 Million) and 79.7% (20.3 Million) of total LBW children respectively, compared to 60% (15.6 Million) as targeted under current 315 districts under Phase-1.
Further, number of common districts (marked in periwinkle) are very less between targeted 315 Phase 1 districts under POSHAN Abhiyaan and bottom 315 district by P (Figure S3). Importantly, these numbers were also lesser when compared with bottom 315 districts based on A (Figure S4). The number of common districts across all three approaches (i.e. 315 POSHAN districts, 315 high burden districts by P and A) are observed to be very few (shaded in black) (Figure S6). For instance, only 65% of targeted 315 districts (under POSHAN Abhiyaan) overlap with those identified as high burden by P and A of child anemia (Table S8). These figures are even lesser in case of LBW (164 districts) (Table S8).
4 Discussion
Our analysis reveals four salient findings. First, a moderate correlation was observed between child undernutrition estimates based on P and A across all districts in India. In addition to this, notable differences were observed in the spatial distribution of failures between tow metrics (P and A). Hence, the disparity between the two metrics indicates that the choice of metric does matter when targeting “sick populations”. Second, the observed correlation between P and A was relatively weaker for LBW and child anemia compared to the correlation for stunting and underweight. Third, substantial variations in district ranking were observed between P and A for all child undernutrition outcomes. In many cases, districts with the highest A were ranked as relatively lower burden districts by P. This reinforces the need to consider both metrics for policy setting and intervention prioritization. Fourth, when targeting child undernutrition, we found a strong correlation of M with both the metrics P and A. Comparison of target coverage across different metrics suggests that M captures relatively higher burden of undernourished children compared to what is being targeted under “Transforming Aspirational Districts” Programme or in phase-1 districts of “POSHAN Abhiyan”.
A clear message emerging from the analysis is that both P and A are important in their own ways as one reflects the ‘risk’ and the other captures the ‘burden’. While we presented the M Index as a way to combine both into one, what is most desirable is to consider them in a combination. In this regard, a typology such as I) high risk/high burden II) high risk/low burden III) low risk/high burden and IV) low risk/low burden, might be more intuitive and respectful of the distinctiveness for policymaking. Figure 1 depicts this typology in a four-quadrant plot. It is clear that quadrants I and IV are straightforward top and least priority districts, respectively. However, prioritization among the middle (quadrants II and III) requires a further contextualization. A potential strategy, for instance, could be to understand the clustering of deprivation in these districts as highly clustered events within a district can provide clear scope for intervention and targeting whereas low clustering would lead to inefficacy in targeting as the event would be spread across the area and may disallow economies of scale in planning and execution.
It may be noted that district ranking can vary substantially across various indicators as well. Differing implications arising from the use of different set of indicators for ranking and assigning priorities can elicit vital information on identifying particular severe cases. For example, mutual exclusive categories of combined nutrition failures—known as composite index of anthropometric failures (CIAF)—by Svedberg (2000) can provide holistic and comprehensive understanding of joint burden across districts. Hence, the importance should also be given to use comprehensive information from different set of indicators.
A moderate concordance between P and A suggests a sense of caution when choosing a metric to target “sick population”. Although this does not indicate the validity or applicability of one metric over the other, it refutes the sole reliance on either one universally. Here, it is worth noting that a high degree of positive correlation was observed between index M with both of the metrics (i.e. P and A). Therefore, the emphasis should be on plurality rather than singularity of metrics, as a metric’s utility depends on the purpose for which it is employed (Subramanian 2005). To place our results in a hypothetical policy scenario, let us suppose a policy objective of allocating funds to establish “Nutritional Rehabilitation Centres” in districts of Sheopur and Gulbarga on the basis of any one metric of stunting. The P metric suggests equal distribution of budget between the two regions since P(Sheopur) = P (Gulbarga) = 52.4%. However, given that the absolute number of stunted children in Gulbarga is about 3.5 times higher than in Sheopur (A(Sheopur) = 51,934 < A(Gulbarga) = 163,463), allocating budget equally in this situation disregards the equity principle. However, index M rightly suggests a substantially higher allocation of resources in Gulbarga than Sheopur as value of M in these districts are 0.292 and 0.165 respectively. The degree of correlation between P and A varied across different indicators of child undernutrition, with relatively weaker correlation for child anemia and LBW. This implies that for different social and health indicators, the choice between P and A can be more consequential. Therefore, the application of any metric for facilitating comparisons or targeting across variable populations must be done in accordance with the precise objective of policy.
The observed differences between district rankings by P and A further support the lack of congruency between the two metrics. In fact, districts with the highest absolute number (A) of undernourished children were not even in the bottom 50% of districts in terms of P (%). The policy implication of this discrepancy becomes clearer when examined in light of the current priority areas identified by the GOI. For instance, the 115 ADs were identified on the basis of a composite weighted index comprising of various indicators (in P) from different development domains (Health and Nutrition, Education, agriculture and Allied, Financial Inclusion, Skill Development, and Basic Infrastructure) (NITI 2018). While the intention and efforts to target vulnerable areas are important and well-placed, the reliance on this sole prevalence-centric index for overall socioeconomic development has severe limitations because district rankings can vary significantly across different development indicators. In fact, if the goal of the ADP is to secure improvements in human development at the national level then it is equally important to consider the metric A.
In addition, we found that only 28 districts were common between the current 115 ADs and the 115 districts we identified as the highest burden areas based on A and M. From our estimates, a simple comparison between the two approaches—when applied to targeting undernourished children in India—indicates that P-based prioritization may miss high-burden areas where substantially higher number of undernourished children are concentrated in India.
The present analysis is not free from certain limitations. First, we have used prevalence estimates from NFHS 2016 to arrive at the absolute numbers of undernourished children using child population data from Census 2011. It may be noted that no latest data on districts-level total child (0–59 months) population was available than Census 2011 and hence the absolute figures could be underestimated. However, it certainly does not affect the distribution of child population across states and districts. Second, we assessed and compared the targets for nutritional indicators only, whereas ADs were identified on the basis of myriad of indicators. A similar exercise can be performed for other development indicators (such as literacy, urbanization, disability, NCDs) in future studies. Third, it should be noted that while this exercise is mostly based on ranking, it does not account for the magnitude of differences in estimates between districts. However, it does not affect the objective of this paper which is to understand the concordance between priority districts between the two metrics (i.e. P and A). While the present analysis can be extended to other programme relevant outcomes particularly those pertaining to mother’s nutritional status (such as low body mass index, and maternal anemia), here we have restricted it to child undernutrition to illustrate the conflicting properties of different metrics.
In this paper, we do not promote the use of one metric over the other. Illustrating why and how the choice of metric matters for policy targeting is central to our study. In fact, studies pertaining to poverty measurements argued that extreme value-orientation to either of the metric should be avoided and prioritization exercise should be broad-based to include alternative perspectives including the choice of metric (P, A or any combination of P and A). Also, the utility of any metric depends on the purpose for which it is employed, and should be based on policy focus and targeting strategy to consider other aspects such as clustering of events to allow for implementation efficiency. For developing populous countries like India which is already grappling with several development problems, such as high level of poverty and illiteracy, maternal and child malnutrition, poor health and health-infrastructure, and intrinsic socioeconomic inequalities, it is critical to adopt appropriate metric for effective targeting and prioritization. The outlined metrics—P, A and M—can be expanded to other indicators to better inform targeting and prioritization mechanisms under diverse social and development policies.
References
Arriaga, E. E. (1970). A new approach to the measurements of urbanization. Economic Development and Cultural Change, 18(2), 206–218.
Besley, T., & Kanbur, R. (1991). The principles of targeting. In Current issues in development economics (pp. 69–90). London: Palgrave.
Bivand, R., & Wong, D. W. S. (2018). Comparing implementations of global and local indicators of spatial association. TEST, 27(3), 716–748. https://doi.org/10.1007/s11749-018-0599-x.
Broome, J. (1996). The welfare economics of population. Oxford Economic Papers, 48(2), 177–193.
Carr-Hill, R. A., & Pessoa, J. (2008). International literacy statistics: A review of concepts, methodology and current data. Montreal: UNESCO Institute for Statistics.
Chakravarty, S. R., Kanbur, R., & Mukherjee, D. (2002). Population growth and poverty measurement (No. 642-2016-44111).
Dandekar, V. M., & Rath, N. (1971). Poverty in India-II: Policies and programmes. Economic and Political Weekly, 6(2), 106–146.
Davis, K., & Hertz, H. (1951). The world distribution of urbanization. Voorburg: International Statistical Institute.
Hassoun, N., & Subramanian, S. (2012). An aspect of variable population poverty comparisons. Journal of Development Economics, 98(2), 238–241.
International Institute for Population Sciences (IIPS) and ICF. (2017). National Family Health Survey (NFHS-4), 2015–16: India. Mumbai: IIPS.
International Institute of Population Sciences. National Family Health Survey, India Mumbai. http://rchiips.org/NFHS/NFHS2016.shtml.
James, S. L., Abate, D., Abate, K. H., Abay, S. M., Abbafati, C., Abbasi, N., et al. (2018). Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. The Lancet, 392(10159), 1789–1858.
Kanbur, R. (2001). Economic policy, distribution and poverty: The nature of disagreements. World Development, 29(6), 1083–1094.
Krtscha, M. (1994). A new compromise measure of inequality. In Models and measurement of welfare and inequality (pp. 111–119). Berlin, Heidelberg: Springer.
Minhas, B. S. (1974). Rural poverty, land redistribution and development strategy: Facts. Indian Economic Review, 1974, 252–263.
Mukherjee, D. (2008). Poverty measures incorporating variable rate of alleviation due to population growth. Social Choice and Welfare, 31(1), 97–107.
NITI Aayog. (2018). Aspirational districts: Unlocking potentials. New Delhi: NITI Aayog, Government of India.
Sen, A. (1976). Poverty: an ordinal approach to measurement. Econometrica: Journal of the Econometric Society, 44(2), 219–231.
StataCorp, L. L. C. (2017). STATA software.
Subramanian, S. (2002). Counting the poor: An elementary difficulty in the measurement of proverty. Economics & Philosophy, 18(2), 277–285.
Subramanian, S. (2005). Fractions versus whole numbers: on headcount comparisons of poverty across variable populations. Economic and Political Weekly, 40(43), 4625–4628.
Subramanian, S., & Mukherjee, D. (2018). On intermediate headcount indices of poverty. Bulletin of Economic Research, 70(4), 443–451.
United Nations Children’s Fund, World Health Organization, The World Bank (2012). UNICEFWHO-World Bank Joint Child Malnutrition Estimates. (UNICEF, New York; WHO, Geneva; The World Bank, Washington, DC; 2012).
von Grebmer, K., Bernstein, J., Hammond, L., Patterson, F., Sonntag, A., Klaus, L., et al. (2018). 2018 Global Hunger Index: Forced migration and Hunger. Bonn and Dublin: Welthungerhilfe and Concern Worldwide.
Zoli, C. (2003). Characterizing inequality equivalence criteria. Mimeo: School of Economics, University of Nottingham.
Zoli, C. (2009). Variable population welfare and poverty orderings satisfying replication properties. Department of Economics (University of Verona) Working Paper, 69.
Acknowledgements
The study was in part supported by Bill and Melinda Gates Foundation, INV-002992. SR and WJ were supported through a grant from Tata Trusts to Institute of Economic Growth, Delhi, India. The authors acknowledge the support of the International Institute for Population Sciences and The DHS Program at ICF (www.dhsprogram.com) for providing access to the 2015–2016 Indian National Family Health Survey data. We are thankful to S. Subramanian for his insightful comments and suggestions.
Author information
Authors and Affiliations
Corresponding author
Additional information
Publisher's Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article's Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article's Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Rajpal, S., Kim, R., Liou, L. et al. Does the Choice of Metric Matter for Identifying Areas for Policy Priority? An Empirical Assessment Using Child Undernutrition in India. Soc Indic Res 152, 823–841 (2020). https://doi.org/10.1007/s11205-020-02467-9
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1007/s11205-020-02467-9